
Infertility is not the end of the road for any woman. Millions of women across India face this challenge quietly, and most cases have a clear medical reason. Understanding the causes of female infertility gives you the power to find the right doctor, ask the right questions, and take real control of your reproductive health before time becomes a concern.
What is Female Infertility
- Female infertility means being unable to get pregnant after 12 months of regular unprotected intercourse for women below 35, or after 6 months for women above 35. The World Health Organization states that roughly 1 in 6 people globally experience infertility at some point. In India, this number is rising due to changing lifestyles, delayed marriages, and increasing daily stress.
- The most reassuring truth is that many causes of infertility are completely treatable when found early. This is exactly why understanding what causes it matters deeply for every woman, whether she plans to conceive soon or simply wants to protect her future reproductive health wisely.
Ovulation Disorders
- The most common cause of infertility in women is difficulty with ovulation. Ovulation is the monthly process of a matured egg being released from the ovary. When this process is irregular, absent, or unpredictable, natural pregnancy cannot happen.
- Polycystic Ovary Syndrome, known as PCOS, is the most widespread ovulation disorder in India, affecting 1 in 10 women of reproductive age. It creates hormonal imbalance that prevents eggs from maturing and releasing properly. Thyroid disorders, both underactive and overactive, disturb the hormonal signals controlling ovulation. High prolactin levels suppress the reproductive hormones needed for regular egg release. Premature ovarian insufficiency, where the ovaries stop functioning before age 40, is another serious reason ovulation fails.
- Warning signs include irregular periods, missing periods for months, very light bleeding, or extremely heavy menstrual flow. A blood test checking FSH, LH, estradiol, AMH, TSH, and prolactin levels identifies most ovulation disorders quickly and accurately.
Blocked or Damaged Fallopian Tubes
- The fallopian tubes are the structures that link the ovaries and the uterus. Their job is to carry the released egg and allow sperm to travel upward for fertilization. When tubes are blocked, narrowed, or damaged by scarring, fertilization inside the body becomes impossible.
- The main cause of tube damage is pelvic inflammatory disease, called PID, which develops from untreated bacterial infections. Sexually transmitted infections like chlamydia and gonorrhea are the leading triggers of PID in young women. Previous ectopic pregnancies, where the fertilized egg implants inside the tube rather than the uterus, cause severe internal tube damage. Past abdominal surgeries can also leave adhesions that block tube function permanently.
- Blocked tubes usually cause no pain or visible symptoms. Most women discover them only during fertility testing. A hysterosalpingography test, known as HSG, uses a dye and Xray to clearly show whether the fallopian tubes are open or blocked. It is a standard and reliable first step in any fertility evaluation.
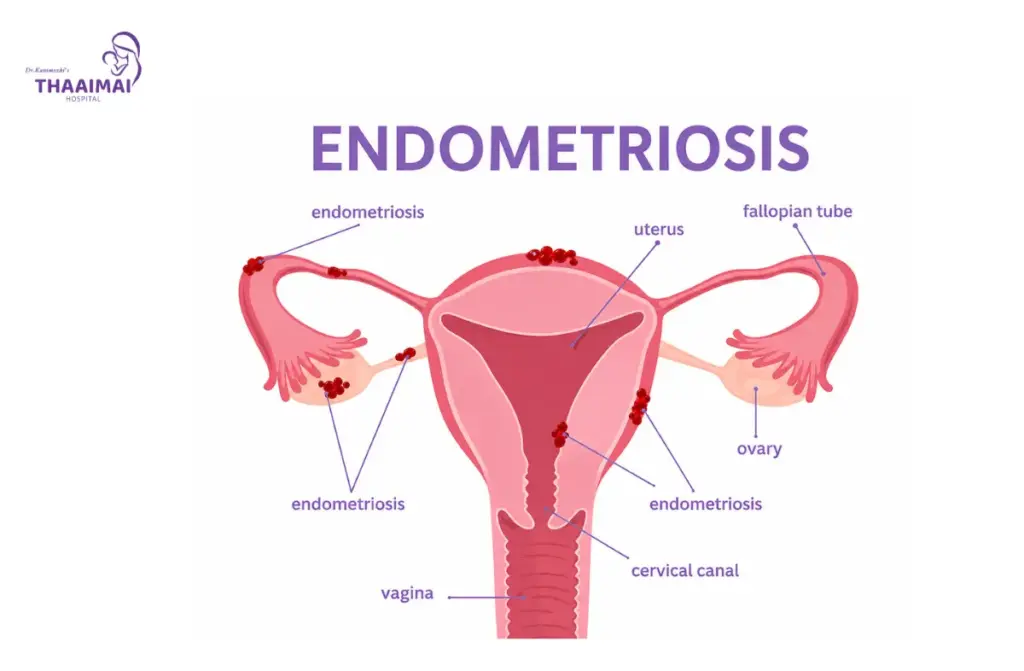
Endometriosis
- Endometriosis is a condition where tissue similar to the uterine lining grows outside the uterus, commonly on the ovaries, fallopian tubes, and pelvic walls. Every month, this tissue thickens and bleeds just like normal uterine lining does. But because it has no exit from the body, it creates internal bleeding, chronic inflammation, painful cysts, and thick scar tissue over time.
- This ongoing internal damage reduces egg quality, blocks tube function, and creates a hostile environment that prevents embryo implantation. Research consistently shows that 30 to 50 percent of women with endometriosis face difficulty conceiving. Common symptoms include severely painful periods, pain during intercourse, chronic pelvic pressure, and unusually heavy bleeding.
- Many women across Tamil Nadu are told that painful periods are completely normal and receive only painkillers without further investigation. If your period pain is severe enough to stop your daily activities or requires you to miss work or school regularly, speak to a gynecologist specifically about endometriosis. Early diagnosis changes treatment outcomes in a major way.
Uterine Problems and Structural Abnormalities
- A healthy uterus is essential for embryo implantation and a successful full term pregnancy. When the structure or lining of the uterus is abnormal in any way, even a perfectly healthy fertilized egg cannot develop into a baby.
- Fibroids are non cancerous muscular growths inside or on the wall of the uterus. Depending on their size and exact location, they can block implantation or reduce blood supply to a developing embryo. Uterine polyps are small soft growths on the inner uterine lining that physically prevent an embryo from attaching properly. A septate uterus is a birth defect where a band of tissue divides the uterine cavity into two parts, making normal pregnancy development very difficult. Asherman syndrome involves scar tissue forming inside the uterine cavity, most often after a dilation and curettage procedure following miscarriage or abortion.
- These conditions are diagnosed through ultrasound and hysteroscopy. Most structural problems can be surgically corrected through hysteroscopy, a minimally invasive procedure requiring no large incision and offering quick recovery.
Age Related Decline in Egg Quality
- Every woman is born with a fixed number of eggs. This number declines continuously throughout life and accelerates sharply after age 35. By the time a woman reaches 40, both the quantity and quality of remaining eggs have reduced considerably.
- Poor egg quality means eggs carry more chromosomal errors. These errors make fertilization harder and significantly increase miscarriage risk even when pregnancy does occur. This is one of the most honest and important causes of female infertility to understand today, especially as more women in Chennai and Tamil Nadu are prioritizing education and career before starting a family.
- An AMH blood test measures the hormone produced by developing egg follicles and gives a reliable estimate of remaining egg supply. Combined with an antral follicle count done through ultrasound, these two simple tests provide a clear picture of your ovarian reserve. Getting this checked in your early thirties provides useful information and options before urgency sets in.
Hormonal Imbalances beyond PCOS
- Several hormonal conditions beyond PCOS affect a woman’s ability to conceive. Insulin resistance, even without a full diabetes diagnosis, creates an environment where the ovaries cannot function normally. High insulin causes the ovaries to produce excess androgens, which are male type hormones that disrupt the egg maturation process directly.
- Adrenal gland disorders that raise androgen levels in the female body interfere with normal follicle development. Low progesterone in the second half of the menstrual cycle means the uterine lining fails to prepare properly for implantation, causing very early pregnancy loss before a missed period is even noticed. Chronic daily stress raises cortisol levels, which suppress the hypothalamus from releasing GnRH, the starting hormonal signal for the entire reproductive chain.
- A detailed hormonal blood panel covering FSH, LH, estradiol, progesterone, testosterone, DHEAS, fasting insulin, and thyroid hormones is one of the most important first investigations when evaluating the causes of female infertility in any patient.
Lifestyle and Environmental Factors
- This cause receives the least attention in public conversations about infertility, yet it is one of the most directly changeable. Daily habits and environmental exposures have a real and measurable impact on female reproductive health.
- Smoking damages egg DNA and reduces ovarian reserve faster than natural aging alone. Even passive smoke exposure affects fertility noticeably. Excessive alcohol consumption disrupts liver function, affecting how reproductive hormones are processed and balanced in the body. Being significantly overweight increases circulating estrogen from fat tissue, which suppresses regular ovulation. Being significantly underweight shuts down the communication between the hypothalamus and ovaries because the body reads very low fat stores as an unsafe state for reproduction.
- Women who follow extreme diets, have eating disorders, or train at very high intensities often experience hypothalamic amenorrhea, where periods stop completely due to hormonal suppression. Exposure to BPA from plastic containers, pesticides from non organic produce, and industrial chemicals in certain workplaces have all been linked to hormonal disruption and reduced fertility in published research. Women in Tamil Nadu working in agriculture or chemical heavy environments should speak to their doctor about possible occupational exposure affecting reproductive health.
Unexplained Infertility
- In approximately 10 to 15 percent of infertility cases, every standard test returns completely normal and no specific cause is identified. This is called unexplained infertility. For couples who have gone through months of testing, this result feels deeply frustrating and discouraging.
- However, unexplained does not mean untreatable. The cause most often exists at a microscopic, genetic, or immunological level that current routine tests cannot yet detect. Advanced investigations such as sperm DNA fragmentation testing, endometrial receptivity analysis, and immune system evaluation can sometimes uncover hidden reasons. Treatments like IUI and IVF have strong and well documented success rates even in unexplained infertility cases. Always seek a second opinion from a reproductive endocrinologist before accepting that nothing more can be done for your situation.
When to See a Doctor
See a fertility specialist if you are below 35 and have been trying for 12 months without success. If you are above 35, do not wait beyond 6 months. If you already have PCOS, thyroid issues, painful periods, a history of pelvic infections, or previous pregnancy loss, consult a gynecologist even before you start trying. Early evaluation gives you more time, more treatment choices, and far more peace of mind. A hormone blood panel, pelvic ultrasound, and HSG tube test together form the most complete and practical starting point for any fertility investigation.
Conclusion
Understanding the causes of female infertility is one of the most empowering things a woman can do for herself. Every cause has a clear path forward when addressed early with the right medical support. The sooner you seek clarity, the more options you have and the stronger your chances of the healthy pregnancy you deserve.